
Length of Hospital Stay: Outpatient
Length of Procedure: Approximately 1 hour
Anesthesia: General with a regional popliteal block
What is Ankle Arthroscopy?
 Ankle arthroscopy is a surgical procedure in which the inside of the ankle joint is examined and treated using a camera and instrumentation that are inserted through small incisions typically one centimeter in length (called portals). Two or three small portals are typically used to perform the procedure.
Ankle arthroscopy is a surgical procedure in which the inside of the ankle joint is examined and treated using a camera and instrumentation that are inserted through small incisions typically one centimeter in length (called portals). Two or three small portals are typically used to perform the procedure.
This minimally invasive technique is useful in treating a number of different problems inside the joint, including sinus tarsi syndrome, scarring, posterior impingement, removal of loose bodies, removal of os trigonum (trigonal process), subtalar fusion, release of the flexor hallucis longus tendon, bursectomy, and removal of Haglund’s deformity.
 Compared to traditional open incisions, the advantages of arthroscopy include earlier rehabilitation, an accelerated rehabilitation course, less pain and blood loss, and a lower rate of infection. Additional procedures may be performed based on the abnormalities found at surgery.
Compared to traditional open incisions, the advantages of arthroscopy include earlier rehabilitation, an accelerated rehabilitation course, less pain and blood loss, and a lower rate of infection. Additional procedures may be performed based on the abnormalities found at surgery.
When the arthroscope is taken out, the incisions are closed using sutures. A boot or splint is applied, and the sutures usually are removed approximately 1 week later.
The Role of Ankle Arthroscopy in the Treatment of Ankle Fractures
The standard treatment for unstable or dislocated ankle fractures is open reduction and internal fixation (ORIF); however, ORIF of ankle fractures has not been associated with “good to excellent” outcomes in all patients in the mid- and long-term. There is evidence that these less than optimal outcomes may be related to intra-articular osteochondral defects (OCD’s). Arthroscopically assisted open reduction and internal fixation (AORIF) provides intra-articular visualization during surgery, which allows for immediate identification of OCD’s, removal of loose bodies, chondroplasty, and/or microfracture, as well as confirmation of successful reduction and fixation of the fractured joint during surgery. There are only two known randomized controlled trials comparing ORIF to AORIF; therefore, the effectiveness of arthroscopy in the treatment of ankle fractures is associated with some controversy.
Thordarson and colleagues (2001) followed 19 patients for 21 months. Nine patients underwent AORIF and 10 patients underwent ORIF. Eight (88.9%) of the AORIF patients had articular damage to the talar dome. After 21 months, AORIF patients had better outcome scores on average; however, this difference was not statistically significant. Given the low numbers of patients in each group, this study has limited power in detecting a difference.
Takao and colleagues (2004) followed 72 patients with an average followup of 3.5 years. In that study, 36 patients with ankle fractures were randomly assigned to each group. 74% of AORIF patients were noted to have an osteochondral defect. The study found that patients who underwent AORIF had significantly better clinical outcome scores than patients who had standard ORIF treatment, but the difference was only 3.4 points on the AOFAS scale on average.
Particularly in higher level injuries, Dr. Carreira has noted arthroscopic assistance to be very useful. In patients who have injuries to the joint in addition to the fractured bones, the arthroscopic treatment may prevent the need for additional future surgeries which may have been treatable at the time of the first surgery.
Video of Ankle Arthroscopy
View additional videos demonstrating rehabilitation and recovery following foot and ankle surgery.
Photo of Plica (Bands of Synovial Fluid)
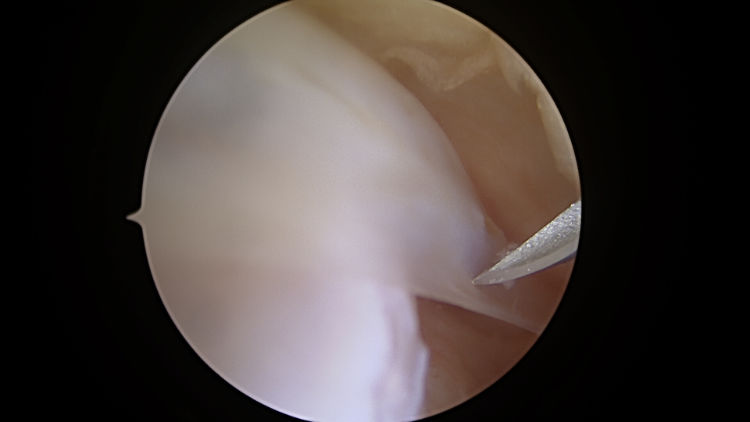
Plica (bands of synovial tissue) noted during a routine ankle arthroscopy.
Risks
The main risks associated with surgery are bleeding, infection, deep vein thrombosis (DVT or blood clot), or damage to superficial nerves of the skin. These risks are very low. Medication, ice, rest, compression, and therapy reduce post operative pain. Complications related to anesthesia are rare but can also occur, as with any surgery. Dr. Carreira may review additional risks with you that are specific to your condition. These risks are lower than with the traditional, larger, open incisions.
Rehabilitation
Our rehabilitation protocol requires strict compliance for optimal results. Weight-bearing as tolerated, Toe-Touch weight-bearing, Partial weight-bearing or Non-weight bearing status will be determined by Dr. Carreira during surgery. The length of protected weight bearing will also be determined at the time of surgery. You will have the aid of crutches, a wheelchair, or roll-about postoperatively for a minimum of 1 week. At your first visit after surgery Dr. Carreira will discuss if physical therapy is needed.
Keep your dressing clean and dry at all times. After your bandage is removed at the first office visit, you may shower as usual. Wash the incision gently with soap and water, pat it dry and apply a clean, dry dressing or Band-aid. No ointments are needed on the incisions.
View additional videos demonstrating rehabilitation and recovery following foot and ankle surgery.
Driving and Flight Information
You will be given a narcotic to help relieve your pain. Legally, you are not allowed to operate heavy machinery (this includes cars!) while on narcotics. Dr. Carreira will discuss return to driving in detail with you at your first visit after surgery.
With regards to flying, during the time that you are not fully weight bearing, precautions should be followed closely to prevent blood clots. This typically includes the use of an injectable blood thinner.
Return to Work
You may return to sedentary work one week after surgery, as long as the pain is well-controlled. However, you must take the time to go to your office visits, and you must follow all post-operative instructions carefully while at work. Returning to heavy labor or sports will be determined by your progression through physical therapy (if needed) and by the extent of damage in your foot.
Follow Up Appointments
Desired appointment intervals for Dr. Carreira’s patients are 2 weeks, 6 weeks, 12 weeks and 6 months.
Always feel free to contact us with your concerns and questions.
Photos of Ankle Arthroscopy




 as seen arthroscopically")






