
Ankle Ligament Reconstruction: What is it?
For Ankle Instability and Ankle Sprain
With twisting injuries of the ankle, the ligaments may be torn and may not heal sufficiently to provide adequate stability in the ankle. Instability of the ankle may show itself in the form of pain or repetitive twisting injuries of the ankle. With each additional sprain that a patient may experience, the ligaments of the ankle can become increasingly loose and dysfunctional. This can result in either chronic pain or repeated twisting episodes. Other associated injuries may also result, including Ankle Cartilage (Osteochondral) Defect, ankle impingement, loose bodies, and peroneal tendon tears. If the twisting episodes are repetitive or if pain persists despite time, conservative treatments such as physical therapy, bracing, medications, and activity modification, then surgery may be an option to help both in the short and long-term.
Office Appointments and Telemedicine with Dr. Carreira
You can also book an office appointment or a telemedicine visit by calling Dr. Carreira’s office at 404-355-0743. Book now.
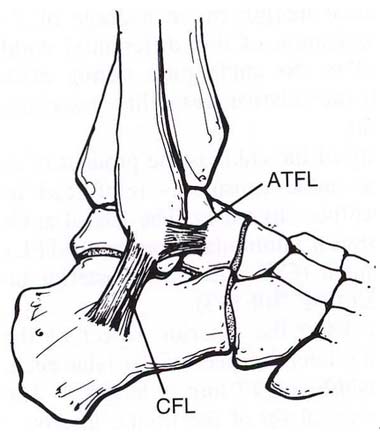
These two ligaments of the lateral ankle are the most frequently injured in the human body. The modified Brostrom technique includes direct anatomic repair of these ligaments. Very small anchors may be drilled into the bone as needed for additional strength. The retinaculum also is incorporated into the repair for additional repair strength.
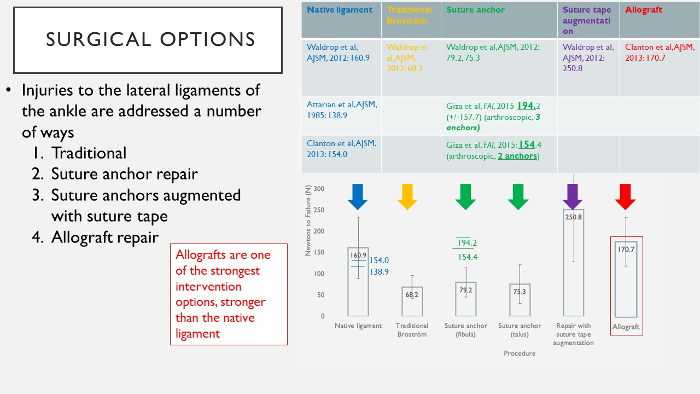
There are several procedures to repair or reconstruct the ankle ligaments, many of which have been studied with clinical outcomes and biomechanical cadaveric studies of strength and stability. Included here are options in Dr. Carreira’s practice.
Video Demonstrating Ankle Instability
In the above video, Dr. Dominic Carreira demonstrates ankle instability while the patient is under anesthesia prior to arthroscopic repair. One can see the amount of translation (movement) that occurs when stressing the ankle, which is excessive. When doing this stress, no translation is normal. Surgical stabilization restores normal stability and is tested routinely at the end of the procedure routinely. (Additional videos about foot and ankle arthroscopy are available on Dr. Carreira’s YouTube channel.)
All Arthroscopic Repair for Ankle Instability
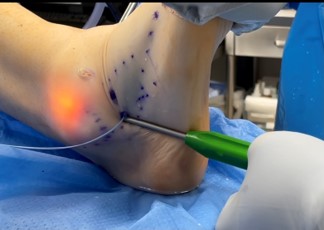
Arthroscopic lateral ligament repair is a minimally-invasive alternative to the open surgery. Dr. Dominic Carreira will create two small holes, one on either side of the ankle, where he will look inside the joint with a scope and insert anchors into the fibula. The anchors are inserted to stabilize the ligaments. All sutures will be passed and tied arthroscopically by making small, 3-4mm incisions as noted below.





After Surgery Recovery Course for Ankle Instability
- Tall CAM boot will be placed immediately after surgery
- Partial weight bearing for the first week after surgery
- Full weight bearing at one week after surgery
- Range of motion at two weeks after surgery: dorsiflexion and plantar flexion only with no inversion or eversion
- Wean out of cam boot at six weeks after surgery
- At six weeks after surgery, transition into an ankle tie up brace for a minimum of six months after surgery and encourage use during sports in the long term
- Plan for return to sport at three months after surgery
Open vs. Arthroscopic Reconstruction with Cadaver Grafting
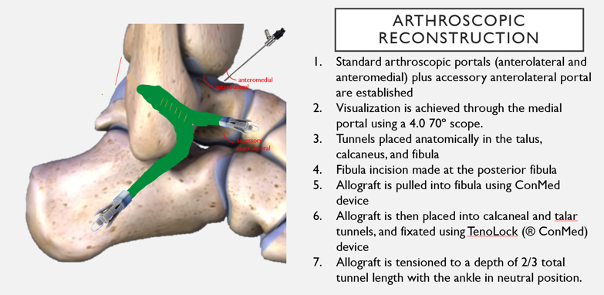
Reasons to consider reconstruction over repair include generalized laxity, increased body weight, high demand level of activity, and previous surgery. These factors are considered on a case by case basis to optimize surgical outcomes. More recently, Dr. Carreira is one of the very few surgeons internationally who performs an all-arthroscopic cadaver ligament reconstruction of the lateral ligaments of the ATFL and CFL. This has the added advantage of being minimally invasive, and may lead to fewer complications, less scarring, and less pain when compared with an open procedure. Dr. Carreira considers all of these factors in his evaluation of whether a particular treatment is right for you.
Arthroscopic Reconstruction
After Surgery Recovery Course for Ankle Instability
Day of Surgery
- A bulky plaster splint is placed
- Ice, elevate, and take pain medication
- Bloody drainage through the splint is expected
- Do not remove the splint but you may add additional ACE wrap bandage
Days 3-5
- First visit to the office
- Change dressings and place in a short leg cast
- Partial weight bearing is allowed
- Elevate the leg regularly to prevent excessive swelling and wound problems
Weeks 2-3
- Sutures removed
- CAM Boot is applied
- Weight-bearing in the boot as tolerated
- The boot may be removed for showering. There is no bathing until the wound is completely healed
- Start ankle up and down motions (dorsiflexion and plantarflexion only) while avoiding heel side to side motions
- Formal physical therapy may be started or delayed until 6 weeks after surgery
6 Weeks
- The CAM boot is weaned to a sneaker-like shoe
- Tie up ankle brace is worn for support for minimum of 6 months
Return to sport typically occurs between 3 and 6 months after surgery, depending on the procedure and any associated injuries treated at the time of surgery.